At the beginning of April last year, just two weeks into our first lockdown, I blogged about the ethics of teaching yoga online, which is, of course, now utterly ubiquitous. I voiced a few concerns, but one thing I was particularly worried about was the ‘[…] potential […] for the personal and commercial exploitation of vulnerability that really needs to be held in our awareness.’ I went on to admonish those who were thinking of profiting from Covid, with my trademark autistic bluntness.
And of course, the subsequent flurry of ‘Yoga for your immune system’ variations on a theme being offered by yoga teachers in classes, workshops and (inevitably) teacher trainings have rather validated my concerns. My ‘Immune Boosting Bullshit’ post explains where I am coming from when it comes to yoga and immunity, but please promise me you’ll read further than my (admittedly pokey) title.
My main concern was that the medical profession at that point, actually knew very little about Covid, what its effects were and how to treat it. So, yoga teachers weighing in with yoga breathing exercises or asanas – for what was assumed at the time to be ‘just’ a respiratory virus – might just have made things worse, not better.
Pivots and Niches

‘Success’ in this whole bullshit profiteering ‘industry’ that I am still part of (often to my own annoyance and surprise) is essentially based on the pivot (that’s business speak for changing your business direction or offering to suit the market) The other thing is niching (which is offer something obscure enough that nobody else does it, but not so obscure that nobody wants it) The best and biggest pivots of this past year have been those that have used Covid-19 situation for niching. And many yoga teachers and wellness types were more than Insta-ready for any self-promotion opportunities that this new niche provided.
I should point out that I don’t object to Yoga for [X condition] from a well-researched therapeutic perspective. I have many brilliant colleagues who offer therapeutic yoga for a range of conditions from a well-evidenced place of solid personal and professional experience. So, having caveated all of that, here we are, a year down the line from voicing those original concerns and (hopefully) anticipating a tentative easing of lockdown. And my yoga ethics antennae are twitching again, with a new crop of ‘offers.’ Yes – the ‘Long-Covid’ class, workshop and CPD workshop/ teacher training is now a thing!
Sigh. Where do I even start?
Maybe a good place to start is to acknowledge – gratefully and soothingly – those of you who have been quietly and tentatively/safely working with Covid Long-Haulers in your communities, for very little money, since it was first identified as a thing. This is not aimed at you.
What do we actually know about Long-Covid?

My own experience of Covid infection in November was unpleasant but relatively short lived. However, my post- Covid symptoms have lasted ever since then, and have included heart palpitations (that I had investigated at A&E) extreme fatigue, insomnia, brain fog, the development of what seems worryingly like sleep apnoea, a strange chronic itch in my ears and persistently weeping eyes.
Interestingly, at no point did I have any breathing issues, a cough, or loss of taste/smell.
The BMJ[i] notes that the range of possible symptoms after acute covid-19 are ‘highly variable and wide ranging’ and lists the most commonly reported symptoms include (but are not limited to):
- Breathlessness
- Cough
- Chest tightness
- Chest pain
- Palpitations
- Fatigue
- Fever
- Pain
- Cognitive impairment (“brain fog,” loss of concentration or memory issues)
- Headache
- Sleep disturbance
- Peripheral neuropathy symptoms (pins and needles and numbness)
- Dizziness
- Delirium (in older populations))
- Abdominal pain
- Nausea
- Diarrhoea
- Anorexia and reduced appetite (in older populations)
- Joint pain
- Muscle pain
- Symptoms of depression
- Symptoms of anxiety
- Tinnitus
- Earache
- Sore throat
- Loss of taste and/or smell
- Skin rashes
If that wasn’t enough, people have also suffered from delayed onset myocarditis[ii] pulmonary embolism[iii] and stroke[iv] following Covid-19 infection. I was checked out for both Myocarditis and PE’s when I presented myself at the Accident & Emergency Department. Thankfully, I didn’t have either of those things, despite feeling pretty lousy.
What I didn’t do was go to a bloody yoga class!
No, I’m not saying that Yoga isn’t helpful
My desire to do anything other than lie down was extremely limited for quite some time. Walking more than a few metres was hard. I cannot discount my experience and understanding of yoga breathing techniques and all of the excellent ways I know to calm my nervous system, including my long-term practice of Yoga Nidra. All of it was hugely helpful. However, the conditions that contribute to Post-Covid syndrome are complex, often severe and still not widely understood. I – despite my long background in therapeutic yoga – would not feel comfortable offering a ‘Yoga for Long-Covid’ class, workshop or anything else.
The reason is, that offering Yoga for [X condition] sets you up as someone who knows about [X condition] Essentially an expert. If your offering is not coming from in-depth personal or professional experience, through training, through years of study and research, then you are not an expert. I am not even sure that there are many medical professionals who would claim to be experts in Long-Covid quite yet.
Hypocrite
In the Yoga for [X condition] conversation, I totally acknowledge my own uncomfortable hypocrisy around the fact that I train yoga teachers to adapt yoga for people living with cancer. I suppose the difference is, cancer has been around for a long time, I have done a lot of study and research, I have had professional training in an oncology setting, many years of practical experience and I have written a book on the subject. I am widely known as a person who knows about yoga and cancer. There is also good clinical evidence for yoga’s efficacy as a supportive therapy for people going through cancer treatment. Even so, I am still learning, and I question constantly whether teaching ‘yoga for cancer’ is actually the right – i.e. ethical – thing to do. For that reason, my course, and my book are built around a solid ethical framework that questions – literally – everything. Especially, and perhaps most importantly, ‘Why are you doing this work?’
It’s just yoga!
Nowadays, yoga that I offer is so integrated, that it could be ‘yoga for cancer’ or it could be…well…just yoga! And yoga should be as accessible to people with cancer or Long-Covid, or any other health issue, as it is anybody else, but the simple truth is, it isn’t.
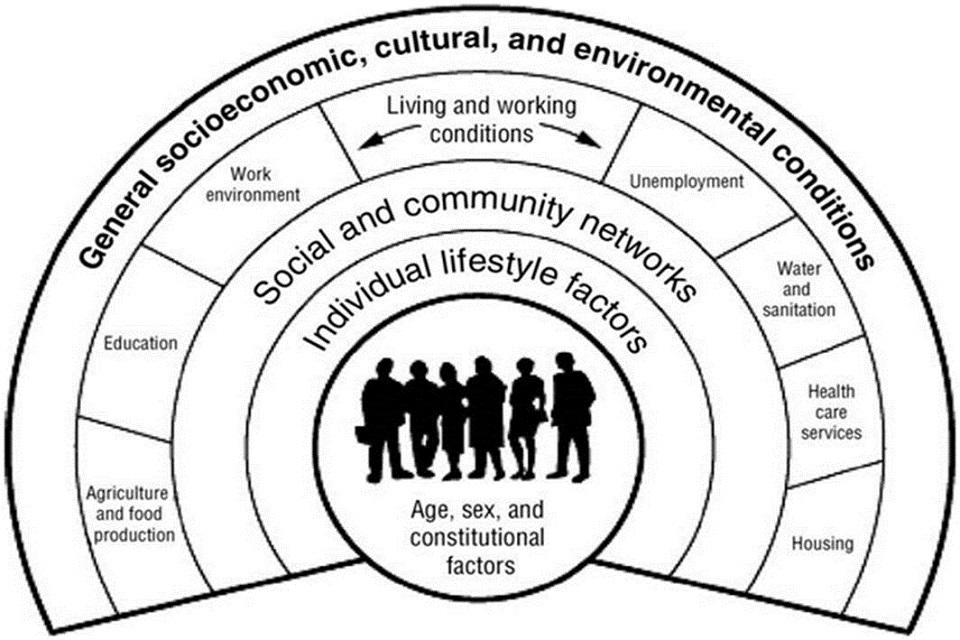
I come back to something I touched on in my last blog post, which is the social determinants of health.[v] Covid and its long- term effects disproportionately affect poor people and people of colour. And these groups of people are hugely unrepresented in yoga spaces. Why? – because those spaces are generally not accessible to them. Yes, I know you may offer your classes free, or on a sliding scale, as I do. But it’s not just about the money! Yoga in the West is a fundamentally white, middle class pursuit. The doing ‘Yoga for’ [X condition] is an incredibly privileged thing to even begin to consider as part of our recovery process from Covid, or anything else.
Yoga probably isn’t that high up the list for most people recovering from Covid. Maybe it should be, who knows? But the necessary, seismic and fundamental release of yoga from the corporate forces of the pivot and the niche, from the incessant monetising of bloody everything that moves, is unlikely to happen any time soon. Tell me I am wrong.
And let’s not forget, that for many in this pandemic, just being alive is a privilege right now.
FOOTNOTES AND REFERENCES
[i] Shah, Waqaar, Toby Hillman, E Diane Playford, and Lyth Hishmeh. 2021. “Managing the Long-Term Effects of Covid-19: Summary of NICE, SIGN, and RCGP Rapid Guideline,” BMJ: n136 10.1136/bmj.n136>
[ii] Bajaj, Retesh, Hannah C. Sinclair, Kush Patel, Ben Low, Ana Pericao, and others. 2021. “Delayed-Onset Myocarditis Following COVID-19,” The Lancet Respiratory Medicine, 0.0 10.1016/S2213-2600(21)00085-0>
[iii] Vadukul, Prakash, Deepak S. Sharma, and Paul Vincent. 2020. “Massive Pulmonary Embolism Following Recovery from COVID-19 Infection: Inflammation, Thrombosis and the Role of Extended Thromboprophylaxis,” BMJ Case Reports CP, 13.9: e238168 10.1136/bcr-2020-238168>
[iv] Perry, Richard J., Craig J. Smith, Christine Roffe, Robert Simister, Saravanan Narayanamoorthi, and others. 2020. “Characteristics and Outcomes of COVID-19 Associated Stroke: A UK Multicentre Case-Control Study,” Journal of Neurology, Neurosurgery & Psychiatry 10.1136/jnnp-2020-324927>
[v] Paremoer, Lauren, Sulakshana Nandi, Hani Serag, and Fran Baum. 2021. “Covid-19 Pandemic and the Social Determinants of Health,” BMJ: n129 10.1136/bmj.n129>
‘All images, except for the social determinants of health, are from Pixabay.
No responses yet